
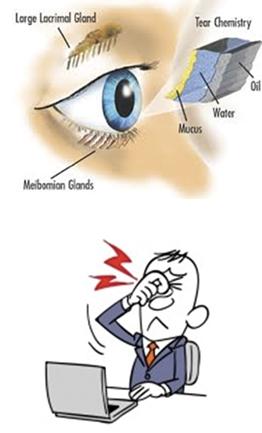
Dry eye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort,visual disturbance and tear film instability, with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.
Dry eye disease is one of the most common ocular complaints. Men and women of 50 years and older have moderate to severe dry eye.
And since tear film is the most anterior surface of the optical system, any irregularities (rapid tear breakup time, for example) can exert considerable impact on visual acuity.
The causes of these symptoms are even more variable and include older age, smoking, contact lens wear, environmental irritants, rosacea, female gender, previous refractive surgery, a variety of medications, certain autoimmune disorders and lacrimal gland trauma.
In some cases, particularly among people who have extended gaze patterns, blinking does not occur frequently enough.
As a result, the tears do not get spread across the eye properly and dry eye occurs. In all cases of dry eye, symptoms may develop or become exacerbated when the weather is windy, the air quality is poor or the humidity is low.
Dry eye symptoms may include redness, itchiness, grittiness, stinging, burning, dryness, excessive tearing, blurry vision, increased blinking, mucous discharge and general discomfort.
New diagnostic methods and equipment are now available:
- Tearosmometer
- Tear MMP-9 immunoassay
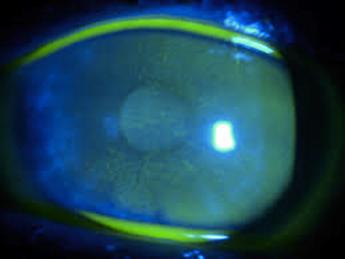
- Tear imaging
- Toninvasive tear break-up test (TBUT)
- Tear stability analysis system
- Oculus keratograph
- Tear interferometry
- Tear meniscus imaging
- Conjunctival cytology, and
- Periodic acid-schiff (PAS) staining
Glaucoma patients under medical therapy may present an exacerbation of dry eye symptoms because of the pharmaceutical agent itself and the preservative agent especially BAK (benzalkonium chloride). This could lead to a deterioration of quality of life of the glaucoma patient.
Patient adherence may be compromised with anti-glaucoma medical therapy, which in turn could lead to a faster progression of glaucoma damage.
An earlier anti-glaucoma surgical approach should be considered in such cases.
Management – Therapy of dry eye syndrome:
- Nonpreserved artificial tear substitutes
- Anti-inflammatory agents
- Tetracyclines (for meibomitis or rosacea)
- Punctal plugs (after inflammation has been controlled)
- Moisture chamber spectacles
If level 2 treatment is inadequate, level 3 measures are added, including the following:
- Autologous serum or umbilical cord serum
- Contact lenses
- Permanent punctal occlusion
